*en inglés
GUILLERMO ROSA-DIEZ 1, GRISELDA BRATTI 1, GRACIELA FILANNINO 3, ADRIANA PEÑALBA 4, FABIÁN OTRERAS 5, MIRIAM LEDESMA 6, MARTÍN ORTEMBERG, GUSTAVO LAHAM 8, MARIANA VÁZQUEZ-DURAND 9, SOLEDAD CRUCELEGUI 1, MARIANO FORRESTER 2, CARLOS MUSSO 1, MARCELO ORIAS 6, RICARDO HEGUILEN 7,
CARLOS DÍAZ 8, RICARDO GARCÍA-MÓNACO 9, OSCAR VELAN 9, HERNÁN TRIMARCHI 2
1 División Nefrología, Hospital Italiano de Buenos Aires, 2 División Nefrología, Hospital Británico, Buenos Aires, 3 Dialiquen S.A, Neuquén, 4 División Nefrología, Hospital Padilla, Tucumán, 5 Instituto Médico San Miguel, Buenos Aires, 6 División Nefrología, Sanatorio Allende, Córdoba, 7 División Nefrología, Hospital José Fernández, Buenos Aires, 8 División Nefrología, CEMIC, Buenos Aires, 9 Departamento de Radiología, Hospital Italiano de Buenos Aires, Argentina
Resumen Prevalencia y factores asociados a calcificaciones vasculares en pacientes con enfermedad
renal crónica en diálisis. El objetivo primario del estudio fue determinar la prevalencia de calcificaciones vasculares en pacientes con enfermedad renal crónica (ERC) en diálisis, a través de métodos accesibles y reproducibles. Como objetivo secundario: determinar los factores de riesgo cardiovascular asociados a la presencia de calcificaciones vasculares y evaluar la utilidad complementaria del ecocardiograma. Fue un estudio prospectivo, transversal y multicéntrico sobre pacientes prevalentes con ERC en diálisis. Se les realizaron radiografía de columna lumbar, de manos y panorámica de pelvis, para la determinación de las escalas de Adragao y Kauppila. La presencia de calcificaciones valvulares fue establecida por ecocardiograma doppler color transtorácico. Se obtuvieron los datos de 30 variables determinadas para el análisis uni y multivariado (regresión logística) de los factores de riesgo asociados. Se evaluaron 443 pacientes adultos de 8 centros de 5 provincias de la Argentina. La prevalencia de calcificaciones vasculares, determinada por las radiografías, fue 63%. La prevalencia de calcificaciones valvulares fue 28%. Las calcificaciones valvulares estuvieron presentes en aquellos pacientes con graves calcificaciones radiológicas. Las calcificaciones estuvieron asociadas a la edad (>55 años), sexo masculino, diabetes, tiempo de diálisis, tabaquismo y la presencia de enfermedad vascular periférica. Este es el estudio con mayor número de pacientes evaluados en Latinoamérica. Se encuentra alta prevalencia de calcificaciones vasculares en Argentina, fácilmente medibles con técnicas no invasivas como la radiografía simple, que resulta más sensible que el ecocardiograma. Ambos estudios deben ser utilizados de manera complementaria.
Palabras clave: calcificación vascular, enfermedad renal crónica, diálisis, Adragao, Kauppila, ecocardiografía
Abstract The main aim of the study was to determine the prevalence of vascular calcifications in patients with chronic kidney disease on dialysis in our population assessed by X-ray. The secondary objectives were to determine the cardiovascular risk factors associated with the presence of vascular calcifications and to evaluate the complementary use of the echocardiogram in a cross-sectional, observational, multicentric study. We included patients with chronic kidney disease on dialysis, age ≥18 years with at least 3 months of renal replacement therapy in 8 dialysis centres in Argentina. The degree of vascular calcification was determined using Adragao and Kauppila scores. The presence of valvular calcifications was established through a trans-thoracic doppler echocardiogram. Univariate and multivariate analysis were undertaken, considering the degree of vascular calcification as the dependent variable; 443 adult patients were evaluated at 8 centres across 5 provinces in Argentina. The prevalence of vascular calcifications by the X-rays was 63%, while 73% presented calcifications in hands and pelvis, with an Adragao score >3, and 60% presented calcifications in the abdominal aorta with a Kauppila score >4. The prevalence of valvular calcifications: 28%. We have shown a higher rate of vascular calcifications with the use of plain X-rays when compared to the prevalence of valvular calcifications obtained with echocardiograms. In this regard, valvular calcifications were present particularly in those patients with a severe level of radiological vascular calcification.
Key words: vascular calcification, chronic kidney disease, dialysis, Adragao, Kauppila, echocardiography
Received: 21-IX-2016 Accepted: 13-III-2017
Dirección postal: Dr. Guillermo Rosa-Diez, Hospital Italiano de Buenos Aires, Juan Domingo Perón 4190, 1199 Buenos Aires, Argentina
e-mail: guillermo.rosadiez@hospitalitaliano.org.ar
Despite therapeutic and technological advances, mortality among patients on dialysis remains very high1. The factors and mechanisms which increase cardiovascular risk in these patients are not entirely known. The main traditional risk factors are age, diabetes, tobacco, dyslipidemia and hypertension. However, individually, these are not enough to account for the increased total cardiovascular risk and the traditional risk scales which apply to the general population are not accurate enough in patients with chronic kidney disease (CKD).
In CKD, malnutrition, inflammation and vascular calcifications clearly emerge among the main non-traditional cardiovascular risk factors. The presence of vascular calcifications in CKD is closely related to mineral and bone metabolism alterations. Once established, vascular calcifications progress with time and are associated to complications such as acute myocardial infarction, ischemic cerebrovascular events and peripheral vascular disease2. A higher prevalence of calcifications in mitral and aortic valves has also been observed in this population. The degree of vascular calcifications and the presence of calcifications in the mitral and aortic valves present a direct correlation to mortality3, 4.
International guidelines5 recommend patients with CKD to be considered at high cardiovascular risk, underscoring the relevance an played in this setting by accurate diagnosis of vascular calcifications.
There are several methods to detect vascular calcifications. The 64-slice multicut computed axial tomography (CAT) is the gold standard and has proven useful when quantifying calcifications both in coronary arteries and in the aorta. However, it is not recommended as a routine technique since it is a sophisticated technique involving high costs and radiation exposure6. A simpler method to diagnose vascular calcifications, which involves less cost and radiation is the plain X-ray of both hands searching for calcifications in the radial and/or interdigital arteries; a pelvic X-ray to study the iliac and/or femoral arteries, and a side view spine X-ray to identify calcifications in the abdominal aorta7.
The presence of vascular calcifications in these X-rays shows a statistically significant correlation with coronary calcifications diagnosed through CAT6-8. Vascular calcifications are observed in the general population and have been considered as an aging-related condition9. In the CKD population, vascular calcifications occur early and rapidly progress in parallel with its high rate of cardiovascular disease. Goodman et al studied the presence of coronary calcification through the electron bean computed tomography technique in patients under 30 years of age in chronic dialysis and found that 80% of them presented calcifications in the coronary arteries10.
The prevalence of vascular calcifications in patients on dialysis in developing countries such as Argentina is barely known. Until recently, in Argentina there was not free access to the recommended drugs, such as calcium-free phosphate binders (sevelamer), vitamin D analogues and calcimimetics, and parathyroidectomy11.
With the purpose of properly evaluating phosphorus calcium metabolism disorders in CKD patients beyond the routine biochemical variables, international guidelines recommend at least one lateral abdominal X-ray to evaluate lumbar aortic calcification or the use of echocardiography for the diagnosis of cardiac valve calcifications, regarding one or the other as a useful and minimally invasive routine alternatives5. However, the complementary use of these techniques has not been evaluated, since the employment of only one of them could result in a sub-diagnosis of extra skeletal calcifications.
Our main goal was to determine the prevalence of vascular calcifications in CKD patients on dialysis in our population by means of the plain X-ray. Our secondary objectives were to determine the cardiovascular risk factors associated to the presence of vascular calcifications and, on the other hand, evaluate the complementary use of echocardiography.
Materials and methods
Cross-sectional, observational, multicentric study. We included all prevalent CKD patients on dialysis, age ≥18 years with at least 3 months of renal replacement therapy (RRT) in 8 dialysis centres in Argentina. An independent ethics committee approved the study.
All patients had lumbar spine and hands X-rays as well as a scan pelvic X-ray to determine the presence and degree of vascular calcification according to the established technique7. The degree of vascular calcification was determined using Adragao12 and Kauppila13 scores. In each center, two physicians determined the degree of calcification for each patient using the same X-rays. One score was made by the treating nephrologist; the other was obtained by the radiologist, who was not familiar with the patient´s history. In order to establish the degree of concordance between the nephrologist and the radiologist, the results were communicated in a double-blind fashion. The presence of valvular calcifications was established through a trans-thoracic doppler echocardiogram.
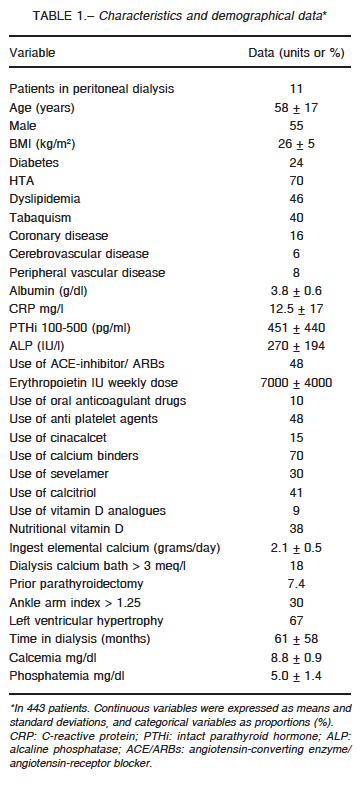
The total calcium intake in the diet was calculated through a diet survey and informed in total grams per week, excluding in the calculation the calcium binders which were included in another variable. The variables included for the analysis of associated risk factors are outlined in Table 1. For the purposes of this study, ischemic cardiopathy was defined as a previous recorded history of documented myocardial angina, acute coronary syndrome or myocardial reperfusion surgery; arterial hypertension was defined as a measurement taken at the initiation of a dialysis session > 140/90 mmHg or the chronic use of antihypertensive medication; dyslipidemia was defined as a total serum cholesterol > 200 mg/dl or the chronic use of hypolipidemic drugs; peripheral vascular disease was defined by the clinical presence of intermittent claudication, limb amputation or an arm-ankle index < 0.9. Results are expressed as the mean plus standard deviation, or median and ranges for the continuous variables according to the statistical distribution of the sample, or in frequencies and proportions for the categorical variables. The prevalence and degree of vascular calcification of our population was established for each of the radiological scores used. An Adragao score higher or equal to 3 or a Kauppila score higher than 4 determined significant calcifications in the analysis of the variables studied. Finally, the prevalence of valvular calcifications was compared between the groups of patients with and without radiological calcification.
The continuous variables were dichotomised to be used in a multivariate model. Univariate analysis (Chi2) and a multivariate analysis (logistic regression) were undertaken, considering the degree of vascular calcification as the dependent variable. A p <0.05 value was considered significant. The Stata 8.0 programme was used for statistical analysis.
Results
A total of 443 patients from 8 centres across 5 provinces in Argentina were evaluated. The demographic characteristics and their variables are shown in Table 1. The 55% were male and the average age was 58 ±17 years; 70% had hypertension and 46% presented dyslipidemia. Diabetes was reported in 24% of the patients and 40% were tobacco-smokers. Time on dialysis was 61 ± 58 months; 7.4% had undergone a parathyroidectomy.
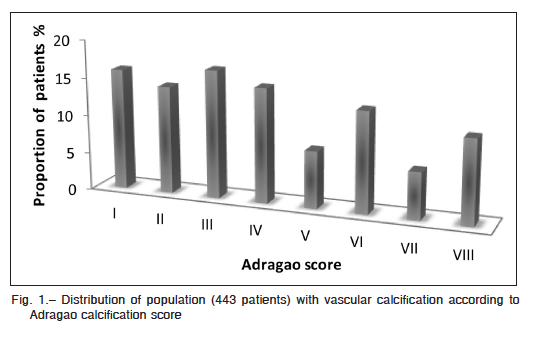
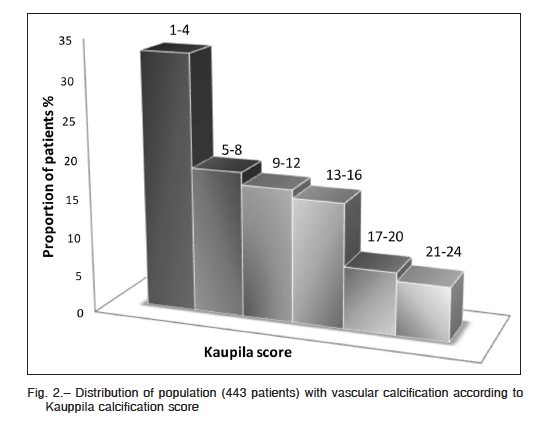
The prevalence of vascular calcifications determined in hands and scan pelvic X-rays, as opposed to the findings in the abdominal aorta X-rays, did not show significant differences (63% and 63.2% respectively). Figures 1 and 2, show the distribution of the population according to the degree of calcification for each score. The 73% of the patients who presented calcifications in hands and pelvis, had an Adragao score higher or equal to 3; 60% of the patients who presented calcifications in the abdominal aorta had a Kauppila score higher than 4.
The prevalence of valvular calcifications was 28%; 32% in patients with an Adragao score higher or equal to 3 and 67% of the patients with a Kauppila score higher than 4. Only 4.5% of the population studied presented valvular calcifications without radiological finding of vascular calcification.
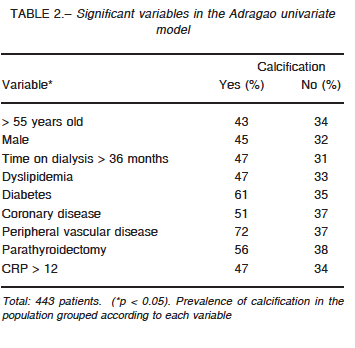
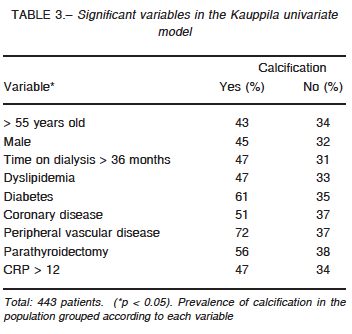
Among all the variables analyzed for the Adragao univariate model, those found to be significant were: age > 55 years, male gender, dialysis therapy >36 months, dyslipidemia, diabetes, coronary disease, peripheral vascular disease, parathyroidectomy and an inflammatory condition, C-reactive protein (CRP) > 12 mg/l) (Table 2). Among the variables analyzed for the Kauppila univariate model, those found to be significant were: age > 55 years, tobacco, dyslipidemia, diabetes, coronary disease and an inflammatory condition (CRP > 12 mg/l) (Table 3). In the multivariate analysis for the Adragao score, the significant variables were male gender (OR 2.04; p 0.006; IC95 1.23-3.39), diabetes (OR 1.73; p 0.024; IC95 1.07-2.79) and time on dialysis (OR 2.11; p 0.018; IC95 1.14-3.91). In the case of Kauppila score, the significant variables were age > 55 years (OR 7.30; p 0.0001; IC 95 3.65-14.6), tobacco (OR 2.13; p 0.016; OR 1.15-3-94) and the presence of peripheral vascular disease (OR 2.24; p 0.027; IC 95 1.10-4.59). The concordance indexes between the nephrologist and the radiologist was 0.85 for the Kauppila score and 0.78 for the Adragao score.
Discussion
In our opinion, this study reports useful information about the prevalence of vascular calcifications in CKD stage VD in a developing country as Argentina. Furthermore, it offers useful information on the different diagnostic methods currently available in developing countries with affordable diagnostic tools.
It is also the largest sample published in Latin America lately. It should be noted that patients undergoing different dialysis modalities have been included14-15.
The prevalence of vascular calcifications was 63% as diagnosed with plain spine, hand and pelvis X-rays.
Publications in the last 10 years have reported 60-90% prevalence depending on the world region analysed and the diagnostic method used. A French paper published by London et al. including 202 patients on haemodialysis with similar dialysis time as ours, also reported 68% prevalence of vascular calcifications diagnosed through X-ray and echocardiogram16. A research paper involving 137 patients in haemodialysis in Australia showed 90% prevalence of abdominal aortic vascular calcification17. Recent reports from Japan and Brazil have separately published 70-80% prevalence of vascular calcifications, but the diagnostic method used in both cases was electron bean computed tomography and not plain X-rays18, 19. The studies involved 50 patients or less, and reported a 50- 60% prevalence of vascular calcifications14-20. Noteworthy, all the mentioned studies presented smaller number of patients and did not include two different dialysis modalities.
The classical vascular risk factors which showed independent association with the presence of vascular calcifications were age, tobacco, dyslipidemia and the presence of peripheral vascular disease, while age was the most significant factor12, 13, 21, 22. With respect to dyslipidemia and inflammation, although not significant in the multivariate model, there was a significant association in both univariate models. Although some papers have shown a significant association between dyslipidemia
and mortality in patients on dialysis, no benefit has been demonstrated with the treatment of hypercholesterolemia in terms of mortality reduction23-26. Coronary artery disease was significant in both univariate models; however, this factor is a consequence or covariable of the classical factors previously mentioned. Time on dialysis was another factor related to the presence of calcifications; in our group over 3 years on dialysis increased the risk of vascular calcifications in a 2-fold manner. This factor has also been recognised as an independent mortality risk27.
There was no association between the use of oral anticoagulation and vascular calcifications. Albeit some clinical reports have shown that oral anticoagulants as vitamin K antagonists are associated with vascular calcifications, the use of vitamin K in patients on hemodialysis did not show to prevent vascular calcifications, Thus, there is not enough evidence yet to recommend vitamin K prescription or the discontinuation of oral anticoagulants to decrease the potential risks of calcification. Some studies using vitamin K in hemodialysis patients are being undertaken to assess its eventual benefit in the prevention of vascular calcifications28.
No differences were found when the two dialysis modalities were compared, i.e. haemodialysis or peritoneal dialysis, both in the univariate or in the adjusted multivariate analyses. This negative data is relevant taking into account the controversies that exist in terms of survival and type of modality29-31 and the fact that there are no reports in the literature comparing the risk of calcification according to the modality employed.
In our cohort, no association was found between the levels of calcium, phosphorus and PTHi, despite 70% of patients presented a calcium daily load of 1.12 ± 0.5 of elemental calcium (following the administration of calcium carbonate or calcium acetate and a 2.6 ± 2.4 gram of total intake (diet + binders)), which was higher than the calcium intake suggested by the K/DOQI guidelines32. Only 30% of the patients were taking calcium free phosphate binders. This lack of association of the biochemical variables and the dietary survey with calcifications is the result of the limitation of a cross-sectional study like this one12, 13, 33, 34.
In our model, previous surgical parathyroidectomy showed a significant association with vascular calcification. Taking into account the fact that PTHi serum levels consistent with a dynamic bone displayed no association with the calcification model, the previous history of surgical parathyroidectomy identified a subgroup of patients exposed to a long time of severe hyperparathyroidism and vascular calcification. In our country, there exists a high prevalence of secondary hyperparathyroidism in patients on dialysis, and the access to surgical treatment was not available until recently11, 35, 36.
Moreover, we have not found any association between the employment of non-calcium based phosphorus binders (sevelamer), vitamin D analogs (paricalcitol) and/or calcimimetics (cinacalcet) and a lower prevalence of vascular calcifications. Noteworthy, in Argentina there was no free access to the above mentioned recommended drugs11. In this regard, it could be argued that the lack of association could be due to a small proportion of patients under these therapies and/or to a short period of time under these drugs.
In this study we have shown a higher rate of vascular calcifications with the use of plain X-rays when compared to the prevalence of valvular calcifications obtained with echocardiograms. In this regard, valvular calcifications were present particularly in those patients with a severe level of radiological vascular calcification. The KDIGO guidelines5 propose either an X-ray of the abdominal aorta or the echocardiogram as the imaging tool for the appropriate evaluation of the calcium-phosphorus metabolic disorders present in CKD. Consistent with our findings, we remark the complementary usefulness of the echocardiogram for the baseline radiologic diagnosis. When possible, both diagnostic methods should be used.
Finally, another important result obtained from our investigation is that after appropriate radiographic techniques and instructions for the search of vascular calcifications employing a quantitative method, semiquantitative results can be achieved as shown by the degree of concordance obtained between the nephrologist who was familiar with the patient´s history and the radiologist (blind arm in the study).
Our work has several limitations, as it consists of a cross-sectional study lacking of biomarkers involved in the physiopathology of vascular calcifications such as FGF23 and fetuin-A37. However, the present study is the first one focused on the prevalence of vascular and valvular calcifications in patients on dialysis in our country. We remark the number of patients included, in addition to the usefulness of a readily available non-expensive diagnostic method as the plain X-ray. Finally, the multi-centric design coupled with the ample regions of the country included and the homogeneous nature of the population under consideration in terms of age and time on dialysis and causes of end-stage renal disease are among the main achievements of our work38.
In conclusion, vascular calcifications are easily assessed in our population on dialysis. Vascular calcifications are easily scored with non-invasive techniques such as the plain X-ray, with an important complementary role played by the doppler echocardiogram. These methods could be used in the screening, diagnosis and treatment-monitoring of calcium-phosphorus disorders in patients on chronic dialysis.
Conflict of interests: None to declare.
References
1. Foley RN, Parfrey PS. Cardiovascular disease and mortality in ESRD. J Nephrol 1998; 11: 239-45.
2. Blacher J, Guerin AP, Pannier B, et al. Arterial calcifications, arterial stiffness, and cardiovascular risk in end-stage renal disease. Hypertension 2001; 38: 938-42.
3. Manjunath G, Tighiouart H, Coresh J, et al. Level of kidney function as a risk factor for cardiovascular outcomes in the elderly. Kidney Int 2003; 63: 1121-9.
4. Wade AN, Reilly MP. Coronary calcification in chronic kidney disease: morphology, mechanisms and mortality. Clin J Am Soc Nephrol 2009; 4: 1883-5.
5. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kid Int 2009; 76: S1-S130.
6. Bellasi A, Ferramosca E, Muntner P, et al. Correlation of simple imaging test and coronary artery calcium measured by computed tomography in hemodialysis patients. Kid Int 2006; 70: 1623-8.
7. Rosa-Diez G., Crucelegui S., Bratti G. et al. Diagnosis of vascular calcification by radiology and semiquantitative methods. Actualizaciones en Osteologia 2014; 10: 82-4.
8. Adar A, Erkan H, Gokdeniz T, Karadeniz A, Cavusoglu IG, Onalan O. Aortic arch calcification is strongly associated with coronary artery calcification. Vasa 2015; 44: 106-14.
9. Wilson PW, Kauppila L, O’Donnel CJ, et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 2001; 103: 1529-34.
10. Goodman WG, Goldin J, Kuizon BD, et al. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med 2000; 342: 1478-83.
11. Douthat WG, Castellano M, Berenguer L, et al. High prevalence of secondary hyperparathyroidism in chronic kidney disease patients on dialysis in Argentina. Nefrologia 2013; 33: 657-66.
12. Kauppila Ll, Polak JF, Cupples LA. New indices to classify location, severity and progression of calcific lesion in the abdominal aorta 25-years follow-up study. Atherosclerosis 1997; 132: 245-50.
13. Adragao T, Pires A, Lucas C, et al. A simple vascular calcification score predicts cardiovascular risk in haemodialysis patients. Nephrol Dial Transplant 2004; 19: 1480-8.
14. Rojas-Campos E, Herrera-Llamas R, Montañez, et al. Vascular calcification in Mexican hemodialysis patients. Arch Med Res 2013; 44: 628-32.
15. Cancela AL, Santos RD, Titan SM, et al. Phosphorus is associated with coronary artery disease in patients with preserved renal function. PLoS One 2012; 7: e36883.
16. London GM, Guerin AP, Marchais SJ, et al. Calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant 2003; 18: 1731-40.
17. Toussaint ND, Pedagogos E, Lau KK, et al. Lateral lumbar X-ray assessment of abdominal aortic calcification in Australian haemodialysis patients. Nephrology 2011; 16: 389-95.
18. Nitta K, Ogawa T. Vascular calcification in end-stage renal disease patients. Contrib Nephrol 2015; 185: 156-67.
19. Barreto FC, Barreto DV, Liabeuf S, et al. Vascular calcification is not an independent predictor of mortality in pre-dialysis adult patients. Nephrol Dial Transplant 2010; 25: 2804-5.
20. Stompór T, Pasowicz M, Sulłowicz W, et al. An association between coronary artery calcification score, lipid profile, and selected markers of chronic inflammation in ESRD patients treated with peritoneal dialysis. Am J Kidney Dis 2003; 41: 203-11.
21. García-Canton C, Bosch E, Ramírez A, et al. Vascular calcification and 25-hydroxyvitamin D levels in non-dialysis patients with chronic kidney disease stages 4 and 5. Nephrol Dial Transplant 2011; 26: 2250-6.
22. Górriz JL, Molina P, Cerverón MJ, et al. Vascular calcification in patients with nondialysis CKD over 3 years. Clin J Am Soc Nephrol 2015; 10: 654-66.
23. Prichard SS. Impact of dyslipidemia in end-stage renal disease. J Am Soc Nephrol 2003; 14: S315-20.
24. Chen HY, Chiu YL, Hsu SP, et al. Association of serum fetuin A with truncal obesity and dyslipidemia in non-diabetic hemodialysis patients. Eur J Endocrinol 2009; 160: 777-83.
25. Müller D, Mehling H, Otto B, et al. Niacin lowers serum phosphate and increases HDL cholesterol in dialysis patients. Clin J Am Soc Nephrol 2007; 2: 1249-54.
26. Joy MS, Dornbrook-Lavender KA. Effects of atorvastatin on Lp(a) and lipoprotein profiles in hemodialysis patients. Ann Pharmacother 2008; 42: 9-15.
27. Ajiro J, Alchi B, Narita I, et al. Mortality predictors after 10 years of dialysis: a prospective study of Japanese hemodialysis patients. Clin J Am Soc Nephrol 2007; 2: 653-60.
28. Caluwé R, Pyfferoen L, De Boeck K, et al. The effects of vitamin K supplementation and vitamin K antagonists on progression of vascular calcification: ongoing randomized controlled trials. Clin Kidney J 2016; 9: 273-9.
29. Beladi Mousavi SS, Hayati F, Valavi E, et al. Comparison of survival in patients with end-stage renal disease receiving hemodialysis versus peritoneal dialysis. J Kidney Dis Transpl 2015; 26: 392-7.
30. Vonesh EF, Snyder JJ, Foley RN, et al. Mortality studies comparing peritoneal dialysis and hemodialysis: what do they tell us? Kidney Int 2006; 103: S3-11.
31. Lukowsky LR, Mehrotra R, Kheifets L, et al. Comparing mortality of peritoneal and hemodialysis patients in the first 2 years of dialysis therapy: a marginal structural model analysis. Clin J Am Soc Nephrol 2013; 8: 619-28.
32. National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003; 42: S1-201.
33. Kwak SM, Kim JS, Choi Y, et al. Dietary intake of calcium and phosphorus and serum concentration in relation to the risk of coronary artery calcification in asymptomatic adults. Arterioscler Thromb Vasc Biol 2014; 34: 1763-9.
34. Guérin AP, London GM, Marchais SJ, et al. Arterial stiffening and vascular calcifications in end-stage renal disease. Nephrol Dial Transplant 2000; 15: 1014-21.
35. Peñalba A, Del Vallae E, Negri A, et al. Parathyroidectomy in chronic kidney disease patients in Argentina: recurrence and persistence. NDT Plus 2011, 4: ii614.
36. Peñalba A, Del Valle E, Negri A, et al. Paratiroidectomía en pacientes renales crónicos en Argentina: estudios prequirúrgicos, tipos de cirujía, recurrencia y persistencia. Rev Nefrologia, Diálisis y Trasplante 2014; 34: 13-20.
37. Schlieper G, Schurgers L, Brandenburg V, Reutelingsperger C, Floege J. Vascular calcification in chronic kidney disease: an update. Nephrol Dial Transplant 2016; 31: 31-9.
38. Marinovich S, Lavorato C, Bisigniano L, et al. Registro Argentino de Diálisis Crónica SAN-INCUCAI 2013. Sociedad Argentina de Nefrología e Instituto Nacional Central Único Coordinador de Ablación e Implante. Buenos Aires, Argentina 2015. In: http://san.org.ar/new/docs/2015/registro_dialisis/registro_ argentinode_dialisis_2013_version_completa.pdf; accessed 05/13/2015.
– – – –
Diciembre 24 [1807] Miércoles, San Gregorio, mártir; vigilia y abstinencia.
El negro Bonifacio Calixto, verdugo de esta ciudad, que gana 150 pesos al año, cometió la fechoría de robar diversos objetos del culto de la iglesia de San Isidro. El Cabildo, en el día de hoy, de acuerdo con la Real Audiencia ha dispuesto que se le descuenten 50 pesos de su suelto.
Alberto M. Salas (1915-1995)
Diario de Buenos Aires 1806-1807. Buenos Aires: Sudamericana, 1981, p 329