
GABRIELA CAEIRO, SILVANA A. ROMERO, SILVANA E. SOLIS, JOSÉ M. POZZI, MARÍA E. LOZANO, JORGE N. WAITMAN
Departamento de Medicina Interna, Servicio de Diabetes, Hospital Córdoba, Córdoba, Argentina
Resumen La vulnerabilidad social ha demostrado ser un factor de riesgo independiente de hipoglucemia en pacientes con diabetes. Los pacientes que se encuentran en situación de vulnerabilidad social reciben asistencia en el sistema de salud pública que brinda atención médica gratuita. Este estudio compara la prevalencia de hipoglucemia en pacientes con diabetes tipo 2 en el sector público frente al privado y su relación con la vulnerabilidad social. Se realizó un estudio multicéntrico descriptivo que incluyó 600 pacientes con diabetes tipo 2 de instituciones de atención pública y privada de Córdoba. El nivel socioeconómico se evaluó a través de la encuesta de la Asociación Argentina de Marketing que evalúa la dimensión social, educativa y económica para estratificar el nivel socioeconómico. Se registró el número de hipoglucemias graves, documentadas sintomáticas y asintomáticas. El 66% de los pacientes pertenecían al sector público. El 41% de los pacientes (n = 246) registró al menos 1 episodio de cualquier evento de hipoglucemia. En el análisis ajustado, se observó un mayor riesgo de hipoglucemia en el sector público (OR 4, 95% CI 2.65-6.04), en pacientes que no tenían educación diabetológica previa (OR 2.28, 95% CI 1.35-3.84), en desempleados (OR 5.04, 95% CI 2.69-9.46) y en aquellos con nivel socioeconómico marginal (OR 60.79 95% CI 14.89-248.13). Factores relacionados con la vulnerabilidad social como el desempleo, el nivel socioeconómico marginal y educación sanitaria deficiente mostraron un aumento en el riesgo de hipoglucemia. Los profesionales que trabajan con personas con diabetes deben tener en cuenta estos factores para un tratamiento seguro de la enfermedad.
Palabras clave: diabetes, diabetes tipo 2, hipoglucemia, poblaciones vulnerables
Abstract Social vulnerability has proved to be an independent risk factor for hypoglycemia in patients with diabetes. In some countries, patients who are in a vulnerable situation are assisted in the public health system which provides free medical care. This study compares the prevalence of hypoglycemia among patients with type 2 diabetes (T2D), in public versus private sector and its relationship with social vulnerability. This multicentric descriptive study included 600 patients with T2D from public and private care institutions of Argentina. Socioeconomic level (SEL) was evaluated through the Marketing Argentinean Association survey. Number of severe, documented symptomatic and asymptomatic hypoglycemias were registered. Among the patients included, 66% were assisted in the public sector. The 41% of patients (n = 246) registered at least 1 episode of any hypoglycemia event being more prevalent in the public sector compared to the private sector (50% vs. 22%). In the adjusted analysis it was observed a greater risk of hypoglycemia in public sector (OR 4, 95% CI 2.65-6.04) and in patients that did not have diabetological education (OR 2.28 95% CI 1.35-3.84). Similarly, unemployment (OR 5.04 95% CI 2.69-9.46), and marginal SEL (OR 60.79 95% CI 14.89-248.13) increased the risk of hypoglycemia. Several factors related to social vulnerability as unemployment, marginal SEL and poor sanitary education showed a significant increase in the hypoglycemia risk. Professionals working with people with diabetes must take into account these factors for a safe treatment of the disease.
Key words: diabetes, type 2 diabetes, hypoglycemia, vulnerable populations
Postal address: Gabriela Caeiro, Hospital Córdoba, Libertad 2051, 5000 Córdoba, Argentina
e-mail: caeirogabriela@hotmail.com
The epidemic of diabetes currently affects lower income populations mainly, increasing not only its prevalence but also the risk of complications 1, 2. It is estimated that 79% of people with diabetes worldwide live in low and medium income countries 3. In Argentina, the prevalence of diabetes is higher in groups of lower income compared to the higher income groups (10.3% vs. 7.3%) 4. Poverty predisposes low socioeconomic level (SEL) people to an inadequate control of their disease since they are in a more vulnerable situation than people of higher income.
Social vulnerability is defined as the reduced ability of a person or group of people to respond (in the sense of cope with, recover from, or adapt to) any external stresses or pressures placed on their livelihoods and well-being 5. This term includes diverse factors such as food insecurity, low SEL, low level of education and a poor sanitary education.
According to studies published to date, social vulnerability has proved to be an independent risk factor for hypoglycemia in patients with diabetes 6. Hypoglycemias are an undesirable effect in the diabetes treatment, which makes this disease control even more difficult.
In our country, the health system is mixed and it comprises three sub-sectors: Public (38% of the population), social security (SS) (46%) and private and prepaid sector (16%). SS includes health insurances, which involucres different types of institutions, such as provincial health care, union health insurances, mixed administration health providers and the Integrated Medical Assistance Program (PAMI for its acronym in Spanish), oriented to retired and pensioners 7-10. Patients who are in a vulnerable situation (unemployed or with informal jobs) have access to the public health system which provides free medical care to people with no health insurance and people who can’t afford to pay one. Instead, the private health care sector (health insurance or prepaid medical care) provides coverage to people with a formal job and with higher SEL in general.
In our knowledge, there are no studies up to date assessing the relationship between hypoglycemia and
socioeconomic factors in patients with diabetes comparing the public and private health sector.
The aim of this work was to compare the prevalence of hypoglycemia among patients with type 2 diabetes (T2D) in the public versus private sector and its relationship with social vulnerability.
Material and methods
A multicentre, analytic, observational, transversal study was conducted in a public Hospital and in private care institutions of Province of Córdoba, Argentina. Ambulatory patients with T2D diagnosis, over 18 years old were included, from January 2nd, 2017 to January 2nd, 2018. Patients with type 1 diabetes (T1D), pregnant and hospitalized patients were excluded.
The following variables were considered: age, sex, time of evolution of the disease, treatment (insulin, sulfonylurea, metformin, incretins, SGLT2 inhibitors), duration of the insulin therapy, weight, height, body mass index, chronic microvascular complications (retinopathy, nephropathy, peripheral neuropathy), macrovascular complications (cerebrovascular accident, acute myocardial infarction and peripheric vascular disease), glycosylated haemoglobin, HbA1c, (measured by methods standardized to the High Performance Liquid Chromatography –HPLC method–), serum creatinine, creatinine clearance calculated by the Modification of Diet in Renal Disease study (MDRD) equation, hypoglycemia prevalence and its causes, previous diabetological education, level of education reached, occupation, medical coverage and SEL.
Data of clinical variables was collected from medical history review.
The social, educational and economic dimension was taken into account to evaluate SEL. This evaluation was done through the Marketing Argentinean Association survey that takes into account occupation of the main income earner, educational level reached, possession of goods and services and type of medical assistance (health care or public sector assistance). The final total score allowed us to include patients in six types of SEL. In our study the classification was simplified in four categories: High, medium (mid-high nd mid-typical) low (superior low category and inferior low category) and marginal SEL 11.
The educational level was categorized according to the maximum educational level reached in two categories: primary level of education or less (illiterate and completed primary) and secondary or more (completed secondary or more). The health care sector was classified in public sector (patients with no health insurance) and private sector (pre-paid medical care and health insurance). Taking into account the occupation, patients were classified as unemployed, employed, retired and pensioner.
Unemployed was defined as any person who, not having an occupation, is actively seeking work. Occupied included all those who were not looking for work and had a stable income. Retired included all those who, having completed the established work cycle, stops working because of his age and receives a pension. Pensioners was defined as anyone who receives non-contributory social security pensions due to disability (people who show a decrease of 76% or more in their work capacity).
Data about hypoglycemia was obtained by self-report during the medical interview and classified in the following way 12: Serious or severe hypoglycemia: event which required a third person’s assistance
Every type of hypoglycemia event: total of the severe and not severe events.
Symptomatic documented hypoglycemia: event with typical symptoms which was confirmed by a blood glucose measure – ment ≤ 70 mg/dl and it was registered in the patient’s diary.
Asymptomatic hypoglycemia: no symptoms appeared, but the blood glucose was ≤ 70 mg/dl and it was registered in the patient’s diary.
The number of severe hypoglycemia episodes within the last 12 months and documented symptomatic hypoglycemia and asymptomatic in the last month was registered during the medical interview.
Presence of diabetic retinopathy (DR) was evaluated though a funduscopy performed by an ophthalmologist. The findings are classified in normal and diabetic retinopathy.
Diabetic nephropathy was evaluated according to urinary albumin-to-creatinine ratio (UACR) measured in isolated urine samples or in 24 hours urine collection. An UACR < 30 mg/g creatinine was classified as norm-albuminuria, between 30-300 mg/g creatinine as micro albuminuria and values > 300 mg/g creatinine as clear proteinuria, for which two measurements are required higher than such values, for the diabetic nephropathydiagnosis 13.
Chronic renal disease was defined in the 3rd stage or based in the glomerular filtration rate of the MDRD formula 14.
Peripheral diabetic neuropathy was established by taking into account the assessment of symptoms and signs by means of the Neuropathy Symptom Scale (NSS) and Neuropathy Disability Score (NDS) where the vibrating, tactile, termoalgesic sensitivity, the muscular strength and the osteotendinous reflexesare evaluated 15.
Presence of macrovascular complications was considered in patients with acute myocardial infarction antecedents, coronary-aortal bypass, percutaneous angioplasty, positive stress test, cerebrovascular accident or peripheral vascular disease history (ABI < 0.9, angiography or revascularization history).
After completing the data sheet from the analysis of medical histories, a descriptive statistics analysis was carried out in accordance with the nature of the variables. For the measurable variables, central and dispersion statistics measures were used (medium, standard deviation); and for the categorical type, the percentage absolute and relative frequencies were studied. For the execution of the inferential analysis the Square Chi test and media differences test were used.
To evaluate independent risk factors, a logistic regression analysis was performed with and without adjustment of variables; Odds Ratio (OR) values were expressed together with their respective 95% confidence intervals (95% CI). Level of significance α = 0, 05 was established. All the analyses were executed with the Stata 14 Software.
The study was approved by the Ethics, Training and Teaching Committee of each of the institutions. All the patients signed the informed consent.
Results
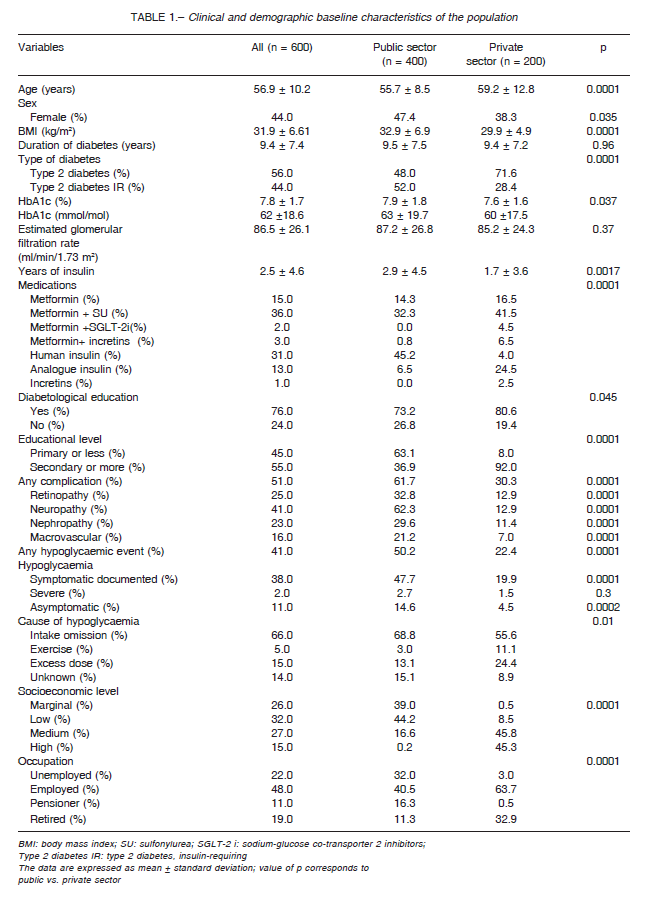
Six-hundred patients with T2D were included, 66% received medical attention in the public sector. The demographic characteristics of the population are detailed in Table 1.
The 41% of the population registered at least 1 episode of any hypoglycemia event (38% a documented hypoglycemia, 2% a severe, and 11% asymptomatic hypoglycemia), being more prevalent in the public than in the private sector (50% vs. 22%). There was a higher frequency of documented symptomatic and asymptomatic hypoglycemia in the public sector compared to the private sector, with no differences in severe hypoglycemia; within the causes of hypoglycemia, the intake omission was more frequent (66%). The intake omission frequency was greater in the public sector compared to the private sector (69% vs. 56%) (Table 1).
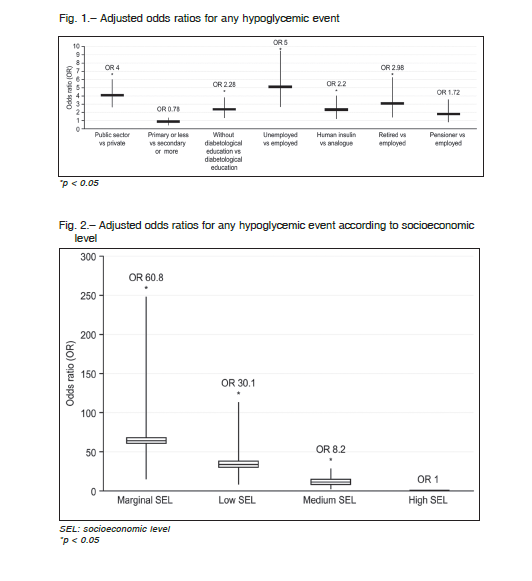
In the adjusted analysis (age, sex, HbA1c, type of diabetes, years of evolution, creatinine clearance and use of insulin) it was observed that patients from the public sector presented greater risk of hypoglycemia compared to the private sector (OR 4.0, 95% CI 2.7-6.0) and those patients that did not have diabetological education presented a greater risk of hypoglycemia (OR 2.3 95% CI 1.3-3.8). Similarly, unemployment increased the risk of hypoglycemia (OR 5.0 95% CI 2.7-9.5) compared with employed people. Among the T2D insulin-treated patients, the ones who received treatment with human insulin presented greater risk of hypoglycemia compared to the ones who received insulin analogues treatments (OR 2.2 95% CI 1.2-4.0). Patients with marginal SEL compared to the high SEL presented greater risk of hypoglycemia (OR 60.8 95% CI 14.9-248.1). However, the low educational level was not associated to hypoglycemia (OR 0.8 95% CI 0.4-1.4) (Figs. 1 and 2).
Discussion
In the last decades, the epidemic of diabetes has taken root in developing world, and it is known that 3 in 4 people with diabetes live in low-medium income countries, an epidemiological trend that will continue increasing in the next years 16. In the same case as with other chronic pathologies, in the case of diabetes, poverty and social exclusion add to the disease a negative effect establishing a vicious circle which worsens health outcomes and affects even more social welfare.
Hypoglycemic episodes are an undesirable effect in the treatment of diabetes, which commonly increase in the desire to diminish the development of chronic complications of the disease. This condition is associated to cardiovascular episodes and cardiovascular death, and also to an increase of morbidity, health expenses and a significant impact in the quality of life, which can worsen the situation of people with this disease 12, 17, 18.
In this study, the frequency of any hypoglycemia episode in T2D was high (41%). Data related to the
prevalence of hypoglycemia in observational studies in T2D are limited and the reports coming from clinical trials that mainly refer to the prevalence of severe hypoglycemia 19-22. In a meta-analysis of 46 clinical trials there was a prevalence of mild and moderated hypoglycemia of 48% and 6% of the severe type 23. The results in Argentina of the Hypoglycemia Assessment Tool (HAT) multinational study informed a prevalence of 48.6% of any type of hypoglycemia episode inT2D treated with insulin 24.
In our study we observed that patients in the public system of health had 4 times more risk of presenting any episode of hypoglycemia compared to private sector, even after adjusting the conventional risk factors of hypoglycemia. Although to our knowledge there are no studies that compare the prevalence of hypoglycemia in sectors of private and public medical care, in a study that evaluated retrospectively the medical consultations in emergency departments due to hypo and hyperglycemic complications over 12 years, it was observed that patients with public health insurance presented twice more consultation rates when compared with patients with private health insurance, and patients who paid out of their own pocket 25. In our setting, patients in the public health sector, have access to the supplies for their treatment through programs that offer therapeutic options less modern like sulfonylureas and human insulin which are associated to a greater risk of hypoglycemia. In this study the use of human insulin increased almost twice the risk of any type of hypoglycemia episode compared to analogue insulin after the adjustment due to confounding variables. Also, patients in the public sector care had lower SEL compared to the private sector. Both variables in this study demonstrated to be independents hypoglycemia risk factors in patients with T2D. These data suggest that the low socioeconomic status could make it difficult for people with diabetes to have access to the necessary supplies for a safer treatment of their disease. Similar data were observed in a greater study available to date, which revealed the risk of severe hypoglycemia in patients with low SEL with T2D taking into account the data obtained from the DISTANCE study. In this study it was observed that those patients with low economic income reported 42% higher risk of severe hypoglycemia compared to those patients with higher economic income26. Similar results were obtained in previously published studies 25, 27-31.
Besides, in the public sector assistance the highest rates of unemployment were recorded in comparison with the private sector. Unemployment in our study proved to be an independent risk predictor for any hypoglycemia episode, increasing 5 times the risk compared to the employed patients. In a study conducted in a public hospital in the province of Córdoba (Argentina), it was found that 46% of patients were unemployed with a 70% more risk of developing hypoglycemia in comparison with the employed patients. The more frequent predisposing factor was the intake omission (57%) suggesting that the budget exhaustion for food can play a role in the incidence of hypoglycaemia 32.
Another component of social vulnerability is the low level of education since these people can have difficulties to understand the correct use of the medication or to know how to prevent hypoglycemia. However, in our study, we did not find a direct association between any hypoglycemia episode and the low level of education.
Although we did not find studies where this aspect is evaluated as a main objective, the existing studies revealed contradictory results. In two post-hoc analysis of the ACCORD study, it was observed that high school education was associated to a higher risk of severe hypoglycemia compared with higher level and graduated education, independently from the treatment group assigned, standard or intensive33-34. Similar results were published in other studies 26, 31, 35. However, other authors did not find such association 36, even in a cohort prospective study, it was observed that the level of education higher that primary was associated to a higher risk of severe hypoglycemias 37.
Taking into account health literacy, we found that the public assistance sector received less previous diabetological education in relation to the private sector. This can be related to the lack of diabetes education programs or difficulty of patients of attending themselves. Patients who did not receive diabetological education had 2 times greater risk of presenting any type of hypoglycemia episode compared to those who received this education, after adjusting due to confounding variables. The limited health literacy is an obstacle for the self-management of the treatment regimens, with less understanding of the instructions, not only of the medicine doses but also of the precautions to take into account, which can lead to an increase in the risk of hypoglycemia. In the DISTANCE 38 study the learning problems, the impossibility to fill out a health questionnaire by themselves and the need of assistance to read the health materials, self-reported by the patients, where connected independently to a severe hypoglycemia risk, between 30-40% greater after the multivariate adjustment. On the other hand, patients who received diabetological education and since they have a better knowledge of the ambulatory management of the insulin therapy and more self-monitoring, have more opportunities to know and treat in an early stage hypoglycemia and mainly to prevent them.
The strengths of this study are the great sample of patients taken from the health system not only public but also private. The transversal cut design is a limitation due to which it is not possible to establish a causal relationship between social vulnerability and hypoglycemia and, thus, the comprehension of the mechanism is still limited.
Furthermore, in this study we have not evaluated one of the most relevant aspects of social vulnerability that is the food insecurity and its possible association with hypoglycemia 39-42 .
Since hypoglycemia together with the social vulnerability constitutes a major barrier for the successful management of the disease, it is essential that these factors are taken into account by the professionals who treat patients with diabetes who are in a vulnerable situation.
Though most of the guidelines currently available imply an individual management of the glycemic objectives, none of them give physicians evidences for the control of these patients 6.
The intrinsic mechanism by which these factors determine a worse control and a greater incidence of hypoglycemia is not clearly defined; due to this fact it will be necessary to carry out long-term prospective studies to discover these aspects and to define strategies to face them.
In conclusion, several factors related to the social vulnerability showed a significant increase in the hypoglycemia risk in these groups of patients. Taking into account this study we can conclude that this increase in the risk might be mainly related to a limited access to the resources for an adequate control of the disease and for the prevention of hypoglycemia. However, more studies are necessary to determine which are the intrinsic mechanisms and the more adequate strategies to reduce the impact. Until then, professionals working with people with diabetes who are in a social vulnerable situation must take into account these factors pointing to their specific needs and giving them easy the access to the necessary supplies for a safe treatment of the disease.
Conflict of interests: None to declare
References
1. Agardh E, Allebeck P, Hallqvist J, Moradi T, Sidorchuk A. Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. Int J Epidemiol 2011; 40: 804-18.
2. Karter AJ, Ferrara A, Liu JY, Moffet HH, Ackerson LM, Selby JV. Ethnic disparities in diabetic complications in an insured population. JAMA 2002; 287: 2519-27.
3. IDF Diabetes Atlas 2017 Update. In: http://www.diabetesatlas.org; accessed September 2019.
4. Ministerio de Salud de la Nación. Tercera encuesta Nacional de Factores de Riesgo para Enfermedades No
Transmisibles. In: http://www.msal.gov.ar/images/stories/publicaciones/pdf/11.09.2014-tercer-encuentro-nacionalfactores-riesgo.pdf; accessed September 2019.
5. Adamo S. Taller Nacional sobre Desastre, Gestión de Riesgo y Vulnerabilidad: Fortalecimiento de la Integración de las Ciencias Naturales y Sociales con los Gestores de Riesgo. Buenos Aires, 31 de Julio de 2012. In: http://moodle.mininterior.gov.ar/biblioteca_dnpc/talleres/adamo_VulnerabilidadSocial_julio31.pdf; accessed September 2019.
6. Berkowitz SA, Aragon K, Hines J, Seligman H, Lee S, Sarkar U. Do clinical standards for diabetes care address excess risk for hypoglycemia in vulnerable patients? A systematic review. Health Serv Res 2013; 48:1299-310.
7. Belló M, Becerril-Montekio V. The health system of Argentina. Salud Pública Mex 2011; 53 suppl 2: S96-108.
8. Gagliardino JJ, Costa Gil JE, Faingold MC, Litwak L, Fuente G. Insulina y control de la diabetes en la Argentina. Medicina (B Aires) 2013; 73: 520-8.
9. Instituto Nacional de Estadísticas y Censos (AR). Beneficiarios de obras sociales por naturaleza institucional. Total del país. Años 2006-2010. In: http://www.indec.mecon.ar/; accessed September 2019.
10. Instituto Nacional de Estadísticas y Censos (AR). Cantidad de obras sociales y beneficiarios, según naturaleza institucional. Total del país. Años 2006-2010. In: http://www.indec.mecon.ar/; accessed September 2019.
11. Índice del nivel socioeconómico 2002. Índice del nivel socioeconómico 2002. Asociación Argentina de Marketing – Cámara de Control y Medición de Audiencias. 2003. Argentina. In: http://www.aam-ar.org.ar; accessed September 2019.
12. Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a report of a workgroup of the
American Diabetes Association and the Endocrine Society. Diabetes Care 2013; 36: 1384-95.
13. American Diabetes Association. Consensus Development Conference on the diagnosis and management of nephropathy in patients with diabetes mellitus. Diabetes Care 1994; 17: 1357.
14. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999; 130: 461-70.
15. Dyck PJ. Approches to improve epidemiological studies of diabetic neuropathy. Diabetes 1997: S5-13.
16. International Diabetes Federation, Diabetes Atlas – Octava Edición, Federación Internacional de Diabetes, Bruselas (Bélgica). In: https://www.idf.org/sites/default/files/attachments/PB_GlobalHealth_ES.pdf; accessed September 2019.
17. Feinkohl I, Aung PP, Keller M, et al. Severe hypoglycemia and cognitive decline in older people with type 2 diabetes: The Edinburgh Type 2 Diabetes Study. Diabetes Care 2014; 37: 507-15.
18. Bloomfield HE, Greer N, Newman D, et al. Predictors and consequences of severe hypoglycemia in adults
with diabetes – A systematic review of the evidence.VA Evidence-based Synthesis Program Reports. Washington (DC): Department of Veterans Affairs, 2012.
19. United Kingdom Prospective Diabetes Study Group: Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatmentand risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837-52.
20. Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008; 358: 2560–72.
21. Duckworth W, Abraira C, Moritz T, et al.; VADT Investigators. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med 2009; 360: 129-39.
22. The Action to Control Cardiovascular Risk in Diabetes Study Group. Effects of Intensive Glucose Lowering in Type 2 Diabetes. N Engl J Med 2008; 358: 2545-59.
23. Edridge CL, Dunkley AJ, Bodicoat DH, et al. Prevalence and incidence of hypoglycaemia in 532,542 people with type 2 diabetes on oral therapies and insulin: a systematic review and meta-analysis of population based studies. PLoS ONE 2015; 10: e0126427.
24. Costa Gil JE, Linari MA, Pugnaloni N, Zambon F, Pérez Manghi F, Rezzónico M. Hipoglucemia en pacientes con diabetes tipo 1 y tipo 2 en tratamiento con insulina. Resultados del Estudio HAT en Argentina. Medicina (B Aires) 2017; 77: 449-57.
25. Ginde AA, Espinola JA, Camargo CA. Trends and Disparities in U.S. Emergency Department Visits for Hypoglycemia, 1993–2005. Diabetes Care 2008; 31: 511-3.
26. Berkowitz SA, Karter AJ, Lyles CR, et al. Low socioeconomic status is associated with increased risk for hypoglycemia in diabetes patients: the Diabetes Study of Northern California (DISTANCE). J Health Care Poor Underserved 2014; 25: 478-90.
27. Booth GL, Hux JE. Relationship between avoidable hospitalizations for diabetes mellitus and income level. Arch Intern Med 2003; 163: 101-6.
28. Wild SH, McKnight JA, McConnachie A, Lindsay RS; Glasgow and Lothian Diabetes Register Data Group.
Socioeconomic status and diabetes-related hospital admissions: a cross-sectional study of people with diagnosed diabetes. J Epidemiol Community Health 2010; 64: 1022-4.
29. Mühlhauser I, Overmann H, Bender R, Bott U, Berger M. Risk factors of severe hypoglycaemia in adult patients with Type I diabetes – a prospective population based study. Diabetologia 1998; 41: 1274-82.
30. Leese GP, Wang J, Broomhall J, et al. Frequency of severe hypoglycemia requiring emergency treatment in type 1 and type 2 diabetes. A population-based study of health service resource use. Diabetes Care 2003; 26: 1176-80.31. Durán-Nah JJ, Rodríguez-Morales A, Smitheram J, Correa-Medina C. Risk factors associated with symptomatic hypoglycemia in type 2 diabetes mellitus patients. Rev Invest Clin 2008; 60: 451-8.
32. Bertola SC, Pozzi JM, Ré DP, Waitman J. Analysis of hypoglycemic events in unemployed patiens. Diabetes 2014; 63: A108.
33. Miller ME, Bond DE, Gerstein HC, et al. The effects of baseline characteristics, glycaemia treatment approach, and glycated haemoglobin concentration on the risk of severe hypoglycaemia: post hoc epidemiological: analysis of the ACCORD study. BMJ 2010; 340: b5444.
34. Punthakee Z, Miller ME, Launer LJ, et al. Poor cognitive function and risk of severe hypoglycemia in type 2 diabetes: post hoc epidemiologic analysis of the ACCORD trial. Diabetes Care 2012; 35: 787-93.
35. Yaffe K, Falvey CM, Hamilton N, et al. Association between hypoglycemia and dementia in a biracial cohort of older adults with diabetes mellitus. JAMA Intern Med 2013; 173: 1300-6.
36. Sonoda N, Morimoto A, Ugi S, et al. Predictors for mild and severe hypoglycemia in insulin-treated Japanese diabetic patients. PLoS ONE 2015; 10: e0130584.
37. Davis TME, Brown SGA, Jacobs IG, Bulsara M, Bruce DG, Davis WA. Determinants of severe hypoglycemia
complicating type 2 diabetes: the Fremantle diabetes study. J Clin Endocrinol Metab 2010; 95: 2240-7.
38. Sarkar U, Karter AJ, Liu JY, Moffet HH, Adler NE, Schillinger D. Hypoglycemia is more common among type 2 diabetes patients with limited health literacy: The Diabetes Study of Northern California (DISTANCE). J Gen Intern Med 2010; 25: 962-8.
39. Seligman HK, Davis TC, Schillinger D, Wolf MS. Food insecurity associated with hypoglycemia and poor diabetes self-managment in a low-income sample with diabetes. J Health Care Poor Underserved 2010; 21: 1227-33.
40. Nelson K, Brown ME, Lurie N. Hunger in an adult patient population. JAMA 1998; 279: 1211-4.
41 Seligman HK, Jacobs EA, Lopez A, Sarkar U, Tschann J, Fernandez A. Food Insecurity and hypoglycemia among safety net patients with diabetes. Arch Int Med 2011; 171: 1204-6.
42. Seligman HK, Schillinger D. Hunger and socioeconomic disparities in chronic disease. N Engl J Med 2010; 363: 6-9.
– – – –
La statistique a cette particularité extraordinaire d´être convaincante même pour des gens qui affirment ne pas la comprendre. «La statistique, pour moi, c´est du chinois». Mais quel non-sinophone serait convaincu par une phrase en chinois ? C´est pourtant là le mystère magique des statistiques : on ne les comprend pas, mais on se soumet à ses conclusions. Je ne sais pas ce que ça veut dire, mais j´y crois. La statistique écrase sous son poids scientifique.
La estadística tiene esta característica extraordinaria de ser convincente incluso para las personas que afirman no entenderla. «Las estadísticas, para mí, son chinos». Pero, ¿qué hablante no chino se convencería con una oración en chino? Este es el misterio mágico de las estadísticas: no las entendemos, pero nos sometemos a sus conclusiones. No sé lo que significa, pero lo creo. La estadística aplasta bajo su peso científico.
Nicolas Gauvit. Statistiques méfiez-vous! Paris: Ellipses Édition Marketing, 2014, p 4